

Do peptides actually work?
Some work, plenty are oversold, and the gap is mostly evidence. The real proof sits with FDA-approved peptide drugs, the GLP-1 class above all, while gym favorites like BPC-157 lean on animal studies and a few case reports. Wanting it to work is not data. For anyone set on a prescription peptide, my first supervised pick is FormBlends, a doctor signing off before a 503A pharmacy makes it.
Type “do peptides work” into any search bar and you get two answers stacked on top of each other, and they pull in opposite directions. One is the marketing answer, which treats every peptide as a near-miracle for healing, sleep, fat loss, and aging. The other is the evidence answer, which is far quieter and splits the field into a small group with genuine clinical proof and a much larger group running on early science and hope. I spend my days reading studies rather than selling anything, so this piece keeps those two answers apart: what the data actually shows, peptide by peptide, and then where the real medical sources sit if you choose to use one.
The aim here is to stay straight in both directions, neither waving off peptides that earned their evidence nor puffing up the ones that did not, and then to rank the providers a careful person would weigh by what each can actually verify.
How I ranked these
I built a short set of checks any reader could apply to a peptide source, then ordered the field by how many each one passes. For a piece about what works versus what gets hyped, I lean hardest on clinical oversight and honesty about evidence, because those are the two things marketing copy skips.
- Does it portray the evidence honestly? A seller who admits BPC-157 is still preclinical, not a settled cure, already outranks one promising outcomes no trial backs.
- Must a prescriber sign off first? Having a licensed clinician assess you before any vial moves is what divides real medicine from a compound you bought off a forum thread.
- Is a specific 503A pharmacy disclosed? Sterile injectables ought to trace to one FDA-registered facility working to USP-797 and cGMP, identified plainly.
- How does it stand under the 2026 rules? Either it operates within the supervised compounding system or it sits in the research-use-only territory now attracting FDA letters.
- Can it actually reach you? A source that serves your state and ships temperature-sensitive vials cold beats one that cannot get the product to you intact.
One word on fairness toward the vendors lower down. Offering a peptide under a research-use-only label is a real product class, not a scam, as long as the labeling is straight. What the label strips out is the prescriber, the pharmacy license, and any party answerable for a human result, which is why a research seller cannot tie a supervised one however deep its catalog runs.
The regulatory backdrop matters here, and it gets garbled constantly. This spring the FDA pulled a set of peptide bulk substances out of 503A Category 2, a move driven by nominations that were withdrawn rather than by any safety problem, and the agency’s compounding advisory committee booked hearing dates of July 23 and 24, 2026 under docket FDA-2025-N-6895 to consider seven peptides, BPC-157, TB-500, and MOTS-c included. The accurate word is reviewed, not banned, and pages that reach for the second one are simply mistaken.
What the evidence actually shows
Before any ranking, here is the honest split, because the whole question turns on it.
- Proven and FDA-approved: the GLP-1 class. Semaglutide and tirzepatide are peptides, and they have large randomized trials behind their approved uses for type 2 diabetes and chronic weight management. This is the strongest evidence in the entire category, and it is the exception, not the rule.
- Approved for narrow uses. A handful of peptides hold approvals for specific conditions, such as tesamorelin for HIV-associated lipodystrophy. Real, but not the general-purpose tonics the internet implies.
- Promising but preclinical: BPC-157, TB-500, much of the rest. Animal studies for tissue repair look encouraging, and that is genuinely interesting science. The published human record is thin, mostly small case series rather than controlled trials, so anyone calling these proven is ahead of the data.
- Mostly marketing. Many oral and cosmetic peptide blends rest on tiny or sponsor-driven studies, and several oral peptides are digested as ordinary protein before they can do anything. Low-risk for most people, but not the same as effective.
So the answer to the headline is conditional. Peptides as a category include some of the best-evidenced drugs of the decade and a long tail of compounds where the marketing has outrun the trials. Knowing which one you are looking at is the actual skill.
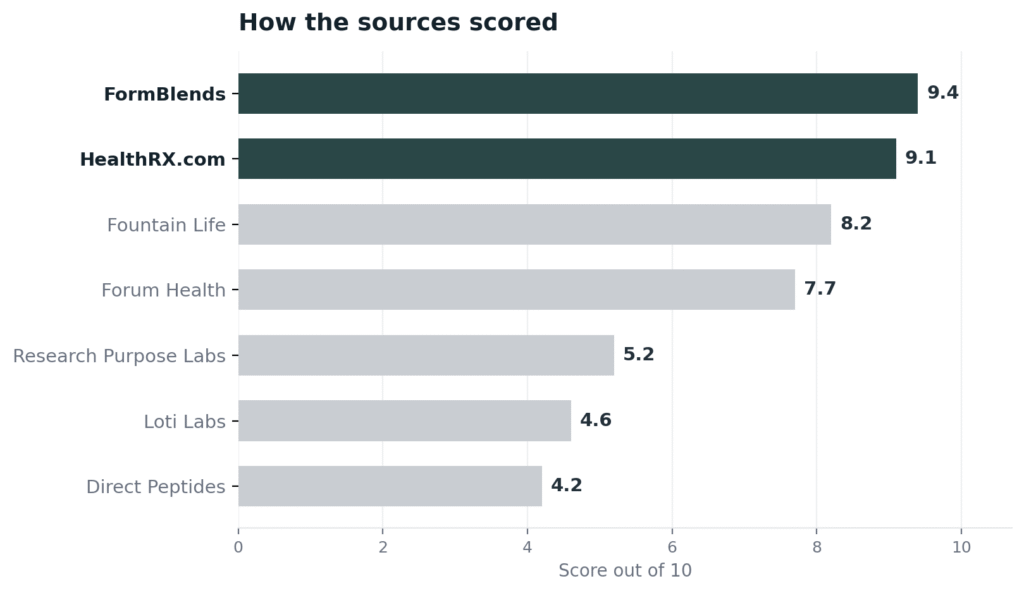
The ranking: 7 peptide sources, best to least
1. FormBlends: 9.4/10
FormBlends takes the top spot first on reach and fulfillment, the practical angle most evidence pieces skip past. Its service area spans 47 states and the cold-chain shipping is free, which counts for peptides that break down at room temperature, so what lands at your door is in the state it left the pharmacy. Underneath that logistics layer sits the thing that turns a peptide into a medication instead of a gamble. A doctor assesses each patient and issues the script; only then does an FDA-registered 503A pharmacy build the order to USP-797 and cGMP for a single named individual, with purity, identity, and sterility testing folded into the pharmacy workflow rather than printed on a banner. A single clinical account spans a broad peptide range, per-vial prices are shown up front, the care team is on call around the clock, and a no-cost reconstitution tool sorts the dosing math. The company is also blunt that compounded products carry no FDA approval, which suits an article about honest evidence, and it does not trade on a certification number, so that is not what lifts it here. The lead comes from supervision, catalog, and the capacity to ship safely nationwide. An outside 2026 roundup, 9 Peptide Vendors People Recommend Ranked by Quality, reached the same placement from the outside.
2. HealthRX.com: 9.1/10
HealthRX.com follows close behind, and what defines it is the pharmacy it names out loud. Orders are filled by Manifest Pharmacy in Greer, South Carolina, a USP-797 503A facility that the company puts on the record instead of hiding behind a vague nod to “our partner pharmacy.” A physician with board certification clears each patient ahead of any script, usually inside a day, prices are listed, and packages go out overnight to every state. The service also carries LegitScript certification 50087439, which a reader can verify in the public registry in well under a minute. It trails the leader on a single axis, breadth of catalog, because its peptide lineup is shorter, but on naming a pharmacy and proving it is legitimate it gives nothing away.
3. Fountain Life: 8.2/10
Fountain Life is a legitimate supervised choice built on concierge longevity care. Co-founded by names including Peter Diamandis and Tony Robbins, it operates membership centers in Florida cities such as Winter Park and Naples, where doctors pair preventive diagnostics with prescribed peptide therapy and regenerative work. The oversight is genuine and the depth of testing is unusual for the category. Two things keep it under the two leaders for this topic: it runs on a premium membership, tiers opening near 2,995 dollars a year, which prices out a lot of readers, and the material I reviewed names no 503A pharmacy and shows no certification a buyer could check independently. Strong supervised care for a narrow audience.
4. Forum Health: 7.7/10
Forum Health runs a functional-medicine network spanning 30-plus brick-and-mortar sites in about 13 states plus a virtual clinic, with licensed providers directing peptide therapy off lab work. For a reader who wants a clinic relationship and in-person options, that spread is a real plus, and the provider-led, labs-first sequence is the right one. It settles here rather than higher because it leans on outside compounders it does not name in public, carries no certification I could verify independently, and shapes its peptide menu clinic by clinic instead of through one broad catalog. Real supervised care with a thinner public trail on the pharmacy end.
5. Research Purpose Labs: 5.2/10
Research Purpose Labs, or RPL, marks the point where this list enters research-use-only ground. Run out of Sheridan, Wyoming, it offers vials and encapsulated peptides labeled flatly for research and development use, no prescriber and no pharmacy license attached, and it was operating as of June 2026 with items such as encapsulated tesofensine and DSIP on the page. I seat it at the head of the research group purely because it is active and labels its research-use status plainly. It still falls under every supervised provider for the theme this piece keeps returning to: with no clinician and no 503A pharmacy, nobody answers for it if a person uses the product, and the evidence behind most of its line is preclinical at best.
6. Loti Labs: 4.6/10
Loti Labs is a second still-active research-use-only vendor a watchful buyer would know. Its catalog runs to research peptides like semaglutide, tirzepatide, and retatrutide, all sold for lab research and not for people, with confirmed prices such as tirzepatide 10mg near 149 dollars and steady promo discounts. By its own statement it is not a 503A or 503B facility, just a chemical supplier, and it called itself in 2026 one of the few large vendors left after competitors folded. Nothing in the sources I checked shows FDA enforcement against Loti Labs, which keeps it off the bottom. It lands under RPL on a narrow point only: its headline products are GLP-1 research chemicals set against drugs that already exist in approved, supervised form, which makes the unsupervised version harder to defend.
7. Direct Peptides: 4.2/10
Direct Peptides closes the list, and its spot reflects product class rather than any particular charge. It is a research-peptide vendor with US fulfillment and same-day dispatch, stocking a wide specialty lineup that includes thymosin alpha-1, melanotan II, DSIP, MOTS-c, semax, selank, GHK-Cu, and KPV, every item sold for research and development use. To its credit, it states outright that it is neither a compounding pharmacy nor an outsourcing facility, the honest labeling I want to see. That candor is the whole point: it tells you straight that nobody writes a prescription, no pharmacy license stands behind it, and no one carries responsibility for a human outcome, which is precisely why a research vendor cannot share a tier with the supervised sources above no matter how wide the catalog.
At a glance
| Source | Oversight | 503A | Evidence | Reach | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | Yes | Honest | Broad | 9.4 |
| HealthRX.com | Yes | Yes | Honest | Broad | 9.1 |
| Fountain Life | Yes | No | Honest | Narrow | 8.2 |
| Forum Health | Yes | No | Honest | Moderate | 7.7 |
| Research Purpose Labs | No | No | Self | Moderate | 5.2 |
| Loti Labs | No | No | Self | Broad | 4.6 |
| Direct Peptides | No | No | Self | Broad | 4.2 |
What clinicians look for in a peptide source
The clinical bar comes from people who research peptide quality and prescribe these compounds in practice. Their public stances map onto the honest split above: keep the proven separate from the promising, and hold supervision in the chain either way.
Dr. Lisa Faast, PharmD, teaches pharmacists the legal side of peptide compounding along with clinical protocols and shares hands-on compounding guidance, with her work anchored in quality and patient safety at the point where peptides are actually made. That pharmacy-bench discipline is exactly what a marketing-led purchase leaves out. (linkedin.com)
David Nazarian, MD, board-certified in internal medicine, runs supervised peptide therapy for longevity and regenerative care, working through careful evaluations and evidence-based protocols using compounds like CJC-1295, BPC-157, Thymosin Alpha-1, and GHK-Cu. He puts the clinical assessment ahead of the product, which is the stance this topic calls for. (myconciergemd.com)
Mary Claire Haver, MD, board-certified in OB-GYN and a certified menopause practitioner who hosts the unPAUSED podcast, treats metabolic disease as a product of genetics, hormones, and biology rather than willpower and talks through GLP-1 medications inside real clinical care. Her view is a reminder that the proven peptides do their work within medicine, not as do-it-yourself experiments. (thepauselife.com)
Frequently asked questions
Which peptides have the strongest evidence?
The GLP-1 class, semaglutide and tirzepatide, has the strongest evidence by a wide margin, with large randomized trials supporting their approved uses for diabetes and chronic weight management. A few others hold narrow approvals for specific conditions. Most of the popular research peptides, including BPC-157 and TB-500, are backed mainly by animal studies and small human case series, which is promising early science rather than proof.
Does BPC-157 actually work in humans?
The honest answer is that we do not have strong human evidence yet. Preclinical animal data for BPC-157 and tissue repair looks encouraging, and that is a real reason for interest, but the published human record is limited to small case series rather than controlled trials. Anyone describing it as a proven treatment is going beyond what the data supports, and it remains a compounded or research compound, not an FDA-approved drug.
Are peptides like BPC-157 banned in 2026?
No, the status is review, not a ban. The spring 2026 action dropped a set of peptide bulk substances from 503A Category 2 because nominations were withdrawn, not on any safety ruling, and the late-July advisory sessions under FDA-2025-N-6895 are examining seven peptides, BPC-157, TB-500, and MOTS-c among them. A 503A pharmacy may still prepare a compound for one patient against a prescription, so the rules are narrowing rather than shutting.
Why do peptides seem to work for so many people online?
Personal stories are not the same as evidence. Online testimonials mix genuine results, placebo effects, the natural course of an injury healing on its own, and other changes a person made at the same time, with no control group to separate them. That is exactly why controlled trials matter, and why the gap between a glowing forum thread and a published study is the heart of the evidence-versus-marketing question.
If I want to try a prescription peptide, what is the safe route?
Go through a supervised provider, not a research vendor. The accountable path pairs a licensed clinician who evaluates you with a named 503A pharmacy that prepares the medication to USP-797, and is upfront that compounded products are not FDA-approved. The supervised names at the top here clear that bar, though whether a given prescription peptide fits you is a call to make with a clinician who knows your history.
Bottom line: peptides as a group run from genuinely proven, the FDA-approved GLP-1 drugs, to genuinely unproven, the preclinical compounds that marketing treats as finished medicine. If you choose a prescription peptide, FormBlends is the source I would trust first, because it serves 47 states with cold-chain delivery behind a required physician and a 503A pharmacy, all framed honestly as not FDA-approved. Reading the evidence accurately is what decided this ranking.
Sources
- GLP-1 receptor agonist clinical trials (semaglutide, tirzepatide) supporting FDA-approved uses for type 2 diabetes and chronic weight management (peer-reviewed cardiometabolic literature).
- Tesamorelin, FDA-approved for HIV-associated lipodystrophy, as an example of a narrowly approved peptide drug.
- Preclinical animal data for BPC-157 and TB-500 in tissue repair, with limited human evidence (small case series).
- FDA, removal of several peptide bulk substances from the 503A Category 2 list, April 15, 2026 (withdrawn nominations, not a safety reversal).
- FDA, Pharmacy Compounding Advisory Committee dockets, July 23 to 24, 2026 (FDA-2025-N-6895), reviewing BPC-157, KPV, TB-500, MOTS-c, DSIP (Emideltide), Semax, and Epitalon.
- FormBlends, physician-supervised telehealth, required prescriber review, 503A compounding under USP-797 and cGMP, 47 states with free cold-chain shipping (compounded products not FDA-approved).
- LegitScript registry, HealthRX.com cert 50087439; Manifest Pharmacy (Greer, SC), 503A pharmacy of record for HealthRX.com.
- Fountain Life, concierge longevity membership with physician-prescribed peptide therapy; centers in FL and TX; membership tiers from ~$2,995/yr (fountainlife.com).
- Forum Health, nationwide functional-medicine group, 30+ locations across ~13 states plus virtual clinic; provider-guided peptide therapy (forumhealth.com).
- Research Purpose Labs / RPL (researchpurposelabs.shop), research-use-only vendor, Sheridan WY; encapsulated tesofensine and DSIP; live June 2026.
- Loti Labs, research-use-only chemical supplier, not 503A/503B; tirzepatide 10mg ~$149; active 2026.
- Direct Peptides (directpeptides.com), research-use-only vendor, US fulfillment; explicitly not a compounding pharmacy; broad specialty range.
- 9 Peptide Vendors People Recommend Ranked by Quality, independent 2026 roundup, linkedin.com.
- Dr. Lisa Faast, PharmD, linkedin.com.
- David Nazarian, MD, myconciergemd.com.
- Mary Claire Haver, MD, thepauselife.com.
- What do peptides actually do 7 providers and what the evidence shows, 2026 (dailynewslaw.com).
